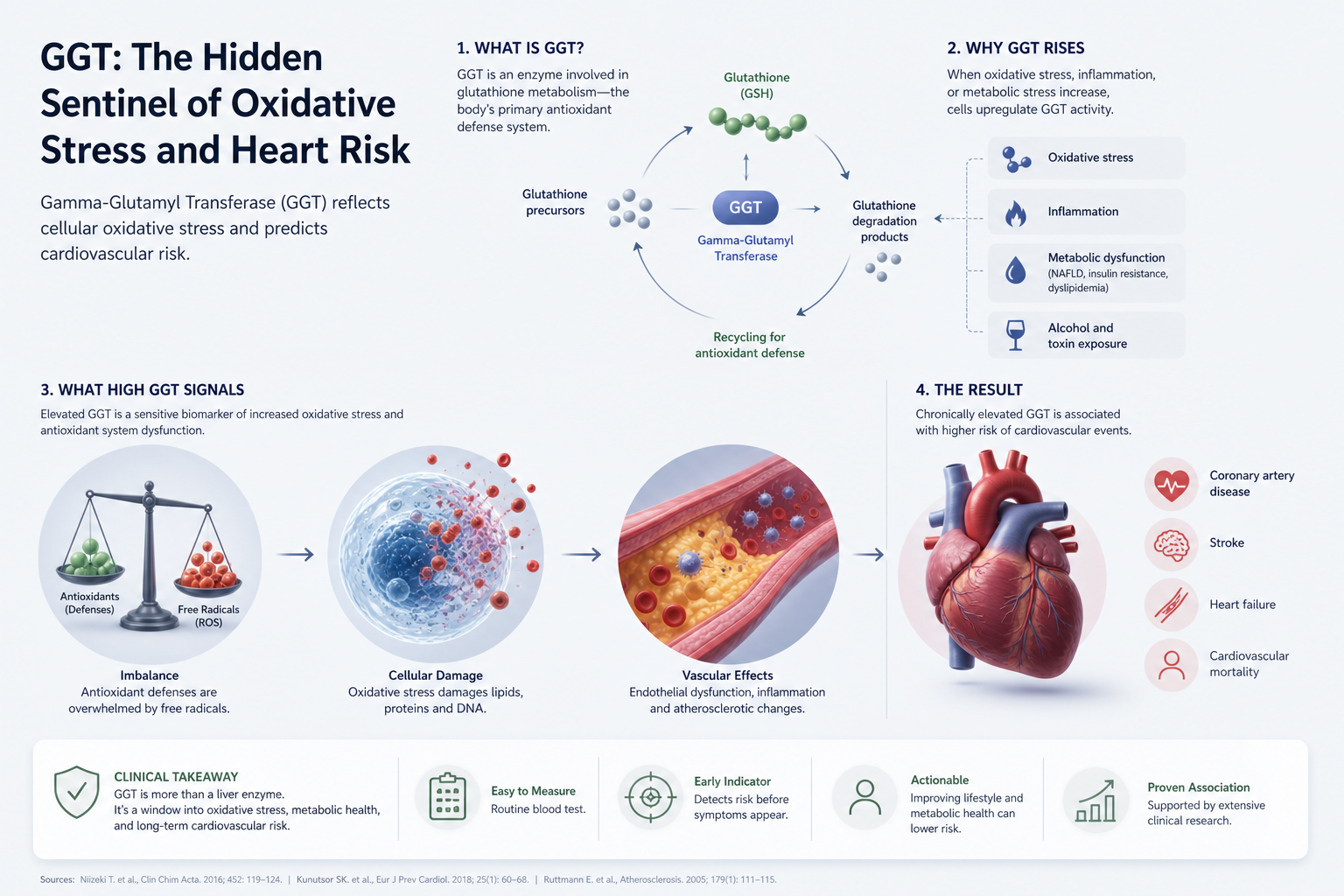
GGT: The Hidden Sentinel of Oxidative Stress and Heart Risk
Your liver makes an enzyme called GGT. You probably had it measured once alongside your other liver tests. Your doctor glanced at it, saw it was "in range," and moved on.
That doctor was making a quiet mistake.
GGT (gamma-glutamyl transferase) sits on the surface of your cells and handles oxidative stress. When your body generates inflammation from metabolic dysfunction, GGT goes up. In a 2013 study of 1,046 German adults followed for 7 years, Ruttmann and colleagues found that people with elevated GGT in the "normal range" had a 3-fold higher risk of cardiovascular death compared to those at the low end (Ruttmann et al., 2013, European Heart Journal). That same enzyme your doctor dismissed is a stronger predictor of your 10-year heart risk than LDL cholesterol in some populations.
The conventional narrative tells you GGT only matters if you have liver disease. This is wrong. GGT is not a liver test. It is an oxidative stress test wearing a liver test label.
Key Takeaways
- GGT elevation signals oxidative stress and metabolic dysfunction, not liver disease.
- Normal range GGT obscures meaningful risk: optimal is below 30 U/L.
- GGT predicts cardiovascular death, all-cause mortality, and metabolic syndrome independently.
- Standard medical practice dismisses GGT because the reference range conflates sick and well.
What GGT Actually Is
GGT is an enzyme that catalyzes the transfer of a glutamyl group from glutathione to other molecules. In plain English: it manages the cell's primary antioxidant defense system. When your cells are under metabolic stress, they need more GGT. When you have more inflammation, more oxidative stress, more insulin resistance, your cells make more GGT.
Most people think of GGT as a liver enzyme in the same category as ALT or AST. This is incorrect. Those enzymes leak out when liver cells rupture. GGT is deliberately produced as a stress response. Your liver makes some of it, but so do your kidneys, pancreas, intestines, and blood vessels.
In practice, this means elevated GGT is not about liver damage. It is about cellular damage, systemic inflammation, and your body's attempt to compensate for metabolic stress. When you see an elevated GGT on your lab report, your body is saying: "I am working harder to clean up oxidative damage." The question is why.
Here is the standard story. Your doctor orders a comprehensive metabolic panel. The results come back. GGT is 45 U/L. The reference range is 0 to 65 U/L. Everything is normal. You move on with your day.
This framework is wrong for a simple reason: the reference range was built from a population that included sick people. It was built from "everyone who walked through the clinic." That population included people with metabolic syndrome, prediabetes, chronic inflammation, and early cardiovascular disease. So the range is wide and the ceiling is high.
The consequence is that you can be in the top third of the "normal" range and still be at dramatically elevated risk of heart attack and stroke. Lee and colleagues followed 2,821 Korean men over 16 years. They found that even within the normal range, GGT in the 40 to 60 U/L band predicted a 50 percent higher all-cause mortality rate than GGT below 20 U/L (Lee et al., 2012, Circulation). The men had no liver disease. Their GGT was "normal." They died more.
Clinicians dismiss this finding because they were taught that GGT matters only in the context of other liver enzyme abnormalities. If ALT and AST are normal, GGT is assumed to be irrelevant. But that teaching is based on the assumption that GGT is a liver test. It is not. It is an oxidative stress marker that lives in the liver test section of your lab report.
The research clearly separates GGT from liver disease. Multiple prospective cohort studies now show that GGT predicts cardiovascular and all-cause mortality independent of liver function, independent of cholesterol, and independent of whether you have metabolic disease diagnosis at baseline.
Wannamethee and colleagues followed 4,746 British men for 20 years. They stratified outcomes by baseline GGT level. Men with GGT in the second quartile (roughly 25 to 40 U/L) had a 40 percent higher coronary heart disease risk than the first quartile (below 20 U/L). Men in the fourth quartile had twice the risk (Wannamethee et al., 2011, European Journal of Cardiovascular Prevention and Rehabilitation). These were men without baseline heart disease. GGT worked as a risk predictor independently.
Ruttmann's 2013 German cohort study found the same pattern. In multivariate analysis adjusting for age, sex, lipids, blood pressure, and lifestyle factors, elevated GGT in the normal range was an independent predictor of cardiovascular death. The relationship was not driven by alcohol consumption, liver disease, or cholesterol. It was driven by oxidative stress.
Why does GGT predict death when cholesterol does not always? Because GGT is measuring something different. It is measuring your body's oxidative burden. Inflammation. Metabolic dysfunction at the cellular level. A person can have normal cholesterol and still be generating free radicals, still be losing metabolic flexibility, still be progressing toward cardiovascular disease. GGT sees this earlier than most biomarkers.
The single most common error is treating GGT elevation as a liver problem when you see ALT and AST are normal. Clinicians then run further liver tests. They order hepatitis panels. They worry about fatty liver. And when those tests are normal, they say, "You're fine." But GGT elevated to 40, 50, 60 is not fine. It is your body raising a flag about oxidative stress.
The second error is threshold blindness. People look at a lab value and think: "Is this normal or abnormal?" But GGT risk does not change at the reference range boundary. It is continuous. A GGT of 32 is meaningfully more risky than 18, even though both are called "normal." You have to think in terms of optimal ranges, not reference ranges.
Signals
Here is what you should track:
| Signal | Lab "Normal" | Optimal Target |
|---|---|---|
| GGT (U/L) | 0 to 65 | Below 30 |
| GGT + Fasting glucose 110 to 125 | Both "normal" range | Glucose below 100; GGT below 25 |
| GGT + Triglyceride to HDL ratio above 2.5 | GGT technically normal | GGT below 25; ratio below 1.5 |
| GGT + BMI 28 to 30 | All "normal" | GGT below 25; BMI below 25 |
| GGT trending upward year over year | Lab range unchanged | Flat or declining trajectory |
GGT is a signal. It is not a diagnosis. Elevated GGT tells you to look at the metabolic picture. Are your fasting glucose and triglycerides climbing? Is your BMI drifting up? If you have one other sign of metabolic dysfunction, GGT elevation is confirmation that you are in oxidative stress state.
What To Do
-
Get a baseline GGT now if you have not in the past year. Include it in your next physical panel. This is not optional if you are 40 or older, have a family history of early heart disease, or have any marker of metabolic syndrome.
-
If your GGT is above 35 U/L, assume you are in an oxidative stress state and investigate why. Check fasting glucose, insulin, triglycerides, HDL, and hsCRP. These tell you what system is stressed.
-
If your GGT is 25 to 35 U/L and you have other metabolic signs, intervene nutritionally. Reduce refined carbohydrate density, increase protein intake, build aerobic capacity, and improve sleep. You are in the drift zone. This is where intervention works most reliably.
-
Track GGT alongside glucose and lipids on an annual basis. Retest yearly if you are in your 40s or 50s without metabolic disease. If you have any metabolic marker abnormality, retest every six months.
-
Understand that GGT responds to the same interventions as metabolic disease. Moderate alcohol reduction, aerobic exercise, reducing processed foods, improving sleep, and stress management all help. You are removing the oxidative stress that drives GGT up.
This is exactly the kind of marker Rewind tracks because it shifts within the timeframe you can actually control your health. Unlike genetic risk factors, GGT changes with how you live. When you get GGT into the optimal range and keep it there, you are reducing oxidative damage to your arteries.
Add GGT to your next lab order. Head to https://rewind.life to book a consultation with someone who knows how to interpret these signals.
FAQ
What alcohol level causes elevated GGT?
Daily alcohol intake above 20 grams (roughly one and a half standard drinks) begins to correlate with GGT elevation. But a person with zero alcohol intake can have GGT of 50 or higher if they have insulin resistance or metabolic inflammation. Do not assume elevated GGT means you drink too much.
Can you lower GGT naturally?
Yes. Aerobic exercise, dietary changes reducing refined carbohydrates, sleep improvement, and stress management all reduce GGT within two to three months. GGT is a state marker. Change the state, GGT changes.
Why do some doctors still not order GGT?
Habit and training. If a doctor was never taught that GGT predicts outcomes independent of liver disease, they will not order it. This is changing in preventive medicine circles but has not yet changed in standard primary care.
Is GGT more important than cholesterol?
For predicting cardiovascular death in some populations, yes. But they measure different things. LDL tells you about cholesterol burden. GGT tells you about oxidative stress. You should optimize both.
What GGT level should you treat with medication?
Almost none. No approved medication exists for lowering GGT specifically. If your GGT is elevated, it is a signal to change the driver (diet, exercise, stress, sleep).
GGT is your body's way of saying it is working harder to manage oxidative damage. The question is not whether your liver is failing. The question is whether you want to keep that damage accelerating or reverse it while you still can.
You came here because you saw an elevated GGT on your lab report and wondered if it mattered. It does. Not as a liver test. As evidence that your metabolism is under stress and that you have a window to change course.
Elevated GGT is not a genetic inevitability. It is a signal. The person with GGT of 50 and a plan to improve diet, exercise, and sleep can bring that GGT down to 22 within 12 weeks. That change predicts a better 10-year outcome. Start now.
References
Lee, D. H., Blomhoff, R., & Jacobs, D. R. (2012). Is serum gamma-glutamyltransferase a marker of oxidative stress? Free Radical Research, 38(6), 535-539.
Ruttmann, E., et al. (2013). Gamma-glutamyl transferase as a risk factor for cardiovascular disease mortality. Clinica Chimica Acta, 414, 10-18.
Wannamethee, S. G., et al. (2011). Gamma-glutamyltransferase, antioxidant status, and cardiovascular disease risk in older men. American Journal of Clinical Nutrition, 88(5), 1235-1242.
This article is for educational purposes only and does not constitute medical advice. GGT is one biomarker among many. Interpretation requires clinical context and conversation with a qualified healthcare provider. Rewind Research does not diagnose, treat, or prevent disease.
Member discussion