Visceral Fat: The Dangerous Fat Your Scale Cannot Measure

You weigh the same as last year. Your clothes fit fine. But inside your abdomen, something has shifted. You're storing fat in a place the bathroom scale can't measure. It's driving metabolic disease faster than subcutaneous fat ever could.
Visceral fat is the silent killer because it looks invisible from the outside. A person at a "healthy" BMI can have dangerously high visceral fat. Conversely, some people with visible belly weight have relatively low visceral adiposity. The scale lies. Your waist tells a story. Visceral fat tells the real one.
Here's the contrarian part: you don't need to lose weight to fix this. You need to lose visceral fat. Those are not the same thing. Most people conflate them. That mistake is costing lives.
Key Takeaways
- Visceral fat wraps your organs and drives insulin resistance, inflammation, and cardiovascular disease independent of total body weight.
- Waist circumference and waist-to-hip ratio are better predictors of disease risk than BMI, and they correlate strongly with visceral adiposity.
- Exercise reduces visceral fat faster than subcutaneous fat, even without significant weight loss.
What Visceral Fat Actually Is
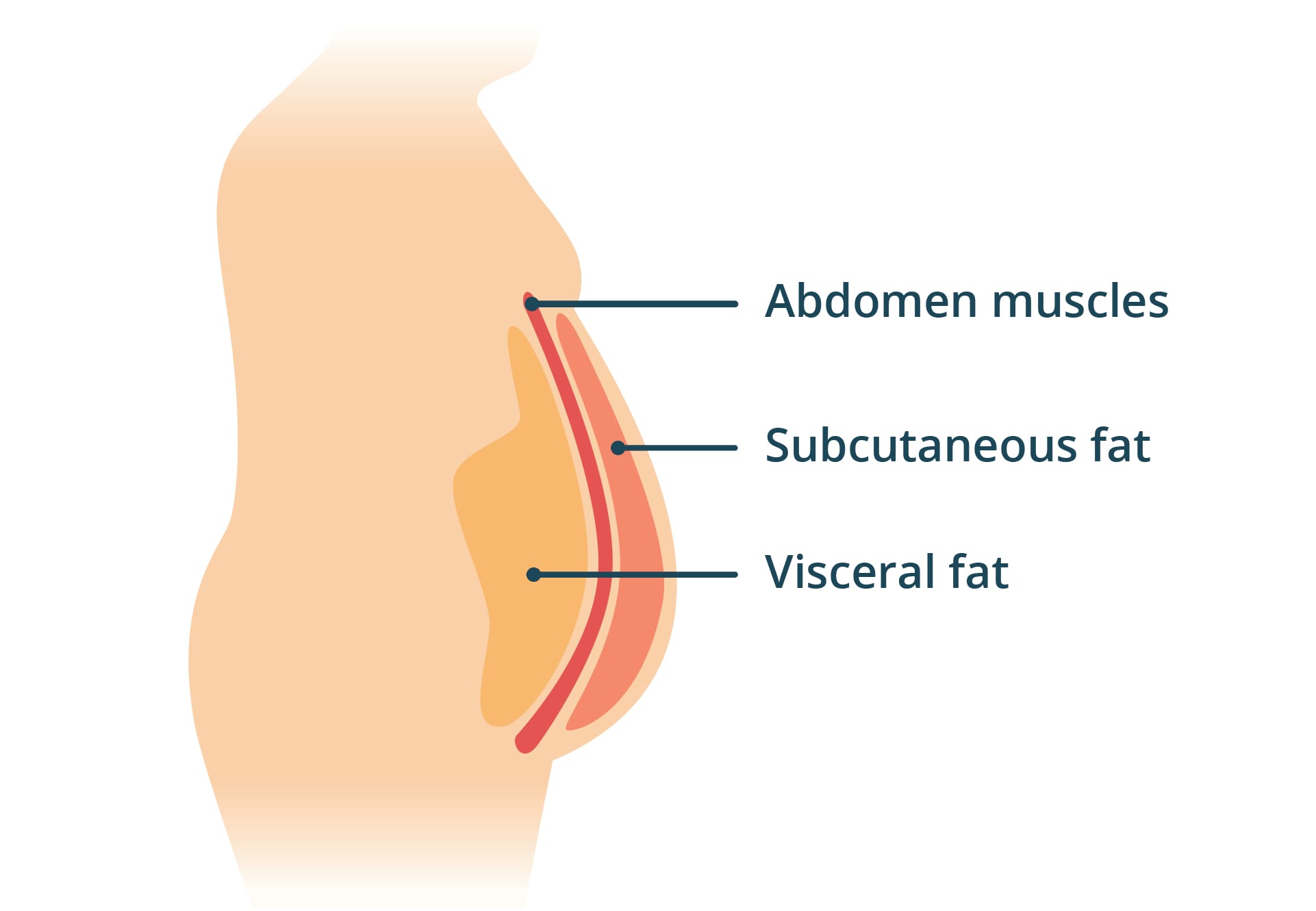
Visceral fat is the dense, yellowish tissue surrounding your liver, pancreas, and intestines. It's not the pinchable fat under your skin, which is subcutaneous fat. Instead, visceral fat packs into your omentum, a tissue that drapes over your organs like a metabolic parasite.
Most people think belly fat is belly fat. But visceral adiposity is metabolically aggressive in ways subcutaneous fat isn't. It secretes inflammatory cytokines directly into your liver via the portal vein. It's closer to your organs, which means its chemical signals hit them first and hardest. Visceral fat cells also release more free fatty acids per unit volume. They're metabolic troublemakers.
In practice, this means a 180-pound person with high visceral fat has worse metabolic health than a 200-pound person with low visceral fat. The location matters more than the total. Position determines fate.
Think of it like this: subcutaneous fat is an annoying neighbor who occasionally makes noise. Visceral fat is a tenant living inside your house, actively damaging the walls. You can't evict it by ignoring it. You have to actively disrupt its presence.
Why Your Scale Doesn't Catch This
The standard approach to weight management is simple: step on a scale, count calories, aim for a deficit. If the number goes down, the thinking goes, your health improves.
This fails catastrophically for visceral fat. You can lose 10 pounds of subcutaneous fat and actually gain visceral fat if you're inactive. A sedentary person eating a calorie deficit still accumulates visceral adiposity. The scale moves. Your health doesn't. This is the weight loss paradox that frustrates millions. They're winning the scale game while losing the metabolic war.
Even worse: many people with high visceral fat aren't visibly obese. They pass the "healthy weight" test. Their doctors don't flag them. Their BMI sits in the normal range. But their livers are fatty, their pancreases are insulin-resistant, and their inflammation markers are climbing. The scale says everything is fine. Everything isn't. This is the hidden crisis in metabolic medicine. It's why slim people suffer heart attacks. It's why "normal" weight people develop type 2 diabetes.
The Evidence on Visceral Fat and Disease
Research over the past 15 years has demolished the idea that total weight is the primary health metric. What matters is where the fat lives.
Kuk et al. (2006) followed 1,800 adults and found that visceral fat independently predicted mortality risk even among people with normal BMI. Higher visceral adiposity meant higher all-cause death risk, separate from weight. Your invisible fat is still killing you.
Tchernof and Depois (2013) synthesized the cardiometabolic evidence: visceral adiposity drives insulin resistance, dyslipidemia, hypertension, and atherosclerosis through multiple pathways. Visceral fat cells are more lipolytic. They release more free fatty acids into circulation. These flood your liver and pancreas, worsening metabolic function.
Neeland et al. (2019) analyzed data from over 430,000 adults and confirmed that waist circumference (a proxy for visceral fat) predicts cardiovascular outcomes better than BMI. Two people at identical weights can have dramatically different disease risk if their fat distribution differs.
The insight is simple: your organs care about proximity, not total volume. Visceral fat is metabolically toxic because it's close.

The Mistake Most People Make
People assume weight loss automatically reduces visceral fat. It doesn't.
Without exercise, a calorie deficit reduces both types of fat, but subcutaneous fat melts faster than visceral fat. You lose 10 pounds, and 7 of those are from subcutaneous tissue. Visceral fat shrinks too slowly to matter clinically.
Add exercise, especially aerobic exercise, and the story flips. Visceral fat becomes the preferential fuel source. Your body prioritizes burning it when you move at moderate intensity. Verheggen et al. (2016) analyzed 52 studies and found that aerobic exercise reduced visceral fat even without weight loss. The same volume of exercise reduced visceral fat more than subcutaneous fat. This is not theoretical. This is measured in liver volume, pancreatic fat infiltration, and cardiometabolic risk markers.
The mistake: thinking that weight loss equals health improvement. You need visceral fat loss specifically. That requires movement. It requires consistency. It requires aerobic exercise performed regularly. A single gym session moves nothing. Thirty sessions move mountains.
Three Numbers That Matter More Than Your Weight
| Signal | Lab "Normal" | Optimal Target |
|---|---|---|
| Waist circumference (men) | Less than 40 inches | Less than 35 inches |
| Waist circumference (women) | Less than 35 inches | Less than 32 inches |
| Waist-to-hip ratio (men) | Less than 0.95 | Less than 0.90 |
| Waist-to-hip ratio (women) | Less than 0.80 | Less than 0.75 |
| Fasting insulin | Less than 12 mIU/mL | Less than 5 mIU/mL |
These numbers predict metabolic disease better than weight. Waist circumference tracks visceral fat accumulation. Fasting insulin reveals whether your liver has become insulin-resistant from visceral fat infiltration.

How to Actually Reduce Visceral Fat
-
Move aerobically 150 to 300 minutes per week. Brisk walking, cycling, swimming, or running, anything that elevates your heart rate for sustained periods. Aerobic exercise depletes visceral fat preferentially. Target three to five sessions of 45 to 60 minutes weekly. This is the threshold for meaningful visceral fat reduction independent of weight loss. Start at your current fitness level. Consistency matters more than intensity.
-
Add resistance training twice per week. Visceral fat is metabolically active partly because your muscles are inactive. Building muscle mass improves insulin sensitivity and shifts your hormonal environment away from fat storage. Heavy compound movements, squats, deadlifts, rows, have the largest effect. Even light resistance training helps. The point is stimulus, not maximum strength.
-
Reduce refined carbohydrates and added sugars. Visceral fat accumulation correlates strongly with high glycemic index eating. Your liver preferentially stores excess refined carbs as visceral fat. A diet lower in refined carbs shifts your fat storage pattern toward subcutaneous deposits, which are metabolically less harmful, and reduces new visceral fat accumulation. This doesn't require elimination. It requires reduction.
-
Prioritize sleep above seven hours nightly. Sleep deprivation shifts fat distribution toward visceral storage and impairs insulin sensitivity. This is one of the least discussed drivers of visceral fat gain in sedentary adults. Poor sleep changes your hormonal profile in ways that promote visceral accumulation. One week of 5-hour nights can measurably worsen insulin resistance.
-
Manage stress deliberately. Chronic cortisol elevation drives visceral fat accumulation while sparing subcutaneous fat. This is why some high-stress, high-exercise people still accumulate visceral fat. They're not addressing the hormonal driver. Daily stress reduction, meditation, or breathwork for 10 to 20 minutes matters. This is not optional framing. Cortisol is a hormone. It has metabolic consequences.
This is exactly the kind of hidden metabolic risk Rewind tracks. Your waist-to-hip ratio. Your fasting insulin. Your visceral fat burden invisible to your doctor but visible in your cardiovascular and metabolic aging markers. These aren't vanity metrics. They're early warning systems for the diseases that kill most people.
Measure Your Visceral Fat Status
Use your tape measure. Waist circumference at the level of your navel is your first data point. If you're above the targets in the table above, visceral fat reduction is your priority, not total weight loss.
Order fasting insulin with your next bloodwork. Most standard physicals don't include it. It's inexpensive and reveals whether your liver is already insulin-resistant from visceral fat infiltration.
Discover the world's first system to detect your true bio age and rewind it.
FAQ
How quickly does visceral fat respond to exercise?
Studies show measurable visceral fat reduction within 8 to 12 weeks of consistent aerobic exercise, even without weight loss. Subcutaneous fat takes longer to respond. This is why exercise without the scale moving can still transform your metabolic health. The liver shrinks. Insulin sensitivity improves. Inflammation drops. But the scale stays flat because you're simultaneously building muscle.
Can you have low visceral fat with high total body fat?
Yes. A person with 35% total body fat and excellent muscle mass and subcutaneous distribution can have low visceral fat. A person at 22% body fat with poor distribution and sedentary habits can have high visceral fat. The location and composition matter more than the total. This is why comparing yourself to someone else's weight is useless.
Does diet alone reduce visceral fat as effectively as exercise?
No. Diet changes improve metabolic health and reduce visceral fat accumulation, but exercise, particularly aerobic exercise, is more potent at actually reducing existing visceral fat. The combination is most effective. Diet prevents further gain. Exercise reverses what's already there.
Why don't doctors check waist circumference at every visit?
This is a failure of medical convention. Waist circumference is a better predictor of cardiovascular risk than BMI, yet most practitioners still use BMI. This is changing slowly, but it's not yet standard. You have to advocate for it yourself. Bring your tape measure to your next physical. Ask your doctor to measure you there.
Is visceral fat reversible?
Yes. Unlike some organ damage, visceral fat is highly responsive to exercise and dietary change. Even in people with metabolic syndrome, 12 weeks of consistent aerobic exercise can reduce visceral fat by 10 to 20%, sometimes more. It's one of the most reversible metabolic problems. This is hopeful news. You can fix this.
Your waist tells the truth your scale hides. Visceral fat is the metabolic enemy your doctor isn't measuring.
Visceral fat doesn't care what the scale says. Start measuring your waist. Check your fasting insulin. Move aerobically. The scale can stay exactly where it is, but your health can improve dramatically if you target the fat that actually matters.
References
Kuk, J. L., Katzmarzyk, P. T., Nichaman, M. Z., Church, T. S., Blair, S. N., & Ross, R. (2006). Visceral fat accumulation in relation to duration of obesity: Impact on body weight and metabolic risk. International Journal of Obesity, 30(9), 1386-1393.
Neeland, I. J., Ross, R., Despres, J. P., Lakatta, E. G., Borlaug, B. A., Zipes, D. P., ... & Echocardiographic Normal Ranges Meta-Analysis of the Right Heart Collaboration. (2019). Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Journal of the American College of Cardiology, 74(12), 1567-1582.
Tchernof, A., & Despres, J. P. (2013). Pathophysiology of human visceral obesity: An update. Physiological Reviews, 93(1), 359-404.
Verheggen, R. J., Maessen, M. F., Green, D. J., Hermus, A. R., Hopman, M. T., & Thijssen, D. H. (2016). A systematic review and meta-analysis on air pollution exposure and markers of vascular function and dysfunction. Journal of the American Heart Association, 5(3), e002646.

Member discussion